The master thesis was written in cooperation with a fitness start-up in Graz and aims to show how several problems can be solved in and after orthopaedic rehabilitation with the help of a fitness and health app (Kendlbacher 2019, 8).
Title Mobile Applikationen in der orthopädischen Rehabilitation
University and year of publication Karl Franzens University Graz, 2019
Level of Design The design of the work itself is structured but no importance was given to making it look appealing – whether colours, additional illustrations, etc. The design of the app (the outcome) is not up to date and is confusing.
Degree of innovation The idea behind a fitness app is nothing new, but the requirements within the app are different, which can increase the degree of innovation. To what extent, I cannot judge.
Independence She wrote her thesis with the support of a start-up in Graz.
Outline and structure She has worked hard on the topic, which is clearly noticeable. She has structured and organised her work into several sections. The work is clearly structured and the division is logical.
Degree of communication It is clearly and simply structured. The author makes it clear what the thesis is about.
Scope of the work The thesis has 76 pages. The scope of the work is large in terms of research, but the design of the app (the final product) is clearly lacking. Unfortunately, the app was not realised but a low fidelity prototype was created and the section describing the app is very small and briefly formulated.
Orthography and accuracy The work is error-free in spelling and comma placement. The language is good. All sources have always been cited. Abbreviations have been marked with a number and described in more detail at the bottom of the page.
Literature The literature varies greatly between years of publication. The paper was published in 2019, there are two sources published in the same year (6 pages of bibliography).
Kendlbacher, Julia. 2019. Mobile Applikationen in der orthopädischen Rehabilitation. Graz: Karl-Franzens-Universität Graz, 2019
My research question at the beginning of the study was whether and how XR can be a help for people with prosopagnosia. Since then, my focus and also my topic for the master’s thesis has changed. The only thing that has stayed the same is that the new topic is also in healthcare. A super short explanation of what future blog posts will be about: For my Master’s thesis, an app is being developed with several people involved and in group work on the topic of preventing dementia. The research topics will revolve around the topics app and dementia.
This first blog entry will be about what aspects we need to consider when designing our app and what points are particularly important to us with regard to the topic dementia and the requirements we received from the project managers. Further blog posts will delve deeper into specific areas. This blog entry is intended as a first start.
User Experience
User experience describes all the impressions and aspects that the user experiences when interacting with a product, like a kind of cycle. The goal should be to make the product (in our case an app) a permanent part of the user’s life. To achieve this goal and start the cycle, the user must first learn about the product, so it means that the presentation of the product must be great. He must be able to immediately understand the benefits that using the app will bring him. The most important thing in the whole cycle is that the user is not frustrated or unnecessarily strained at any time. Otherwise, the product may not be used. (cf. Schilling, Apps machen, 37).
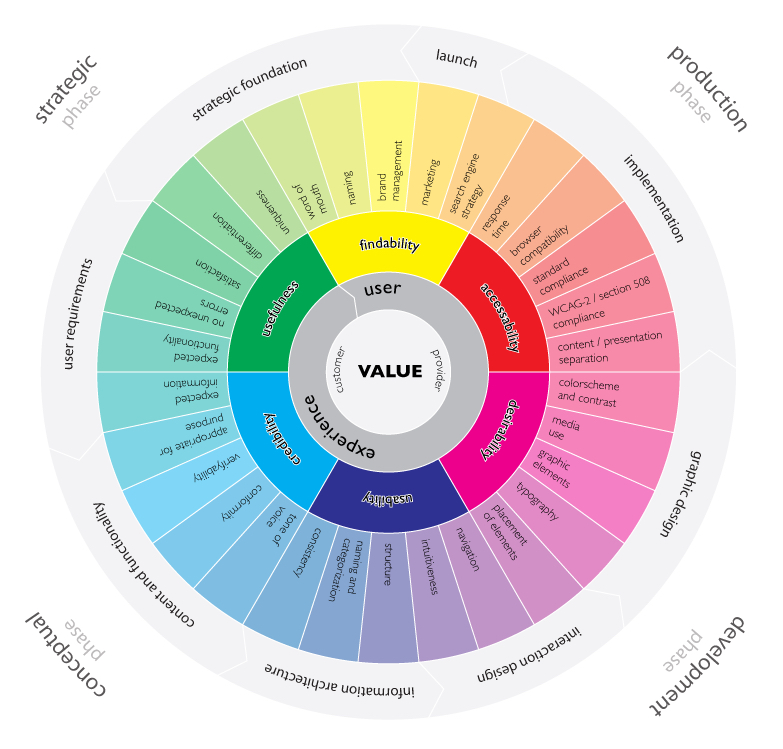
This infographic by Magnus Revang breaks down the user experience design process into several phases. It is intended to answer the question “what is user experience? (Revang, The User Experience Wheel). The model starts with the word ‘value’ in the middle and implies that for both the providers of the product and the customers, the product’s goal is to create added value and thus it can bring benefits to both groups. The six coloured words are defined terms that should be focused on most. The 30 words are factors that contribute to a positive user experience (cf. Revang, The User Experience Wheel).
The User Experience Wheel (Magnus Revang)
2. Three states of an Appscreen
When designing an app, three conditions must always be considered and observed (cf. Basecamp, Getting Real, 48):
What does the screen look like normally, when everything works and the action can be carried out
How the screen looks empty, without data
What does the screen look like when an error message appears
The blank screen at first use is especially important. If this screen is not adequately considered, it can lead to the app not being used or the user being frustrated because they do not know what task they have to complete. Examples of how to fill this page are instructions, help texts, example screens, FAQ, explanations of how the screen looks filled in and so on (cf. Basecamp, Getting Real, 49).
3. Important factors to consider
Efficiency when using the app
Efficiency when using the app
User satisfaction during use
What the app should do must be clearly defined
Navigation within the app must make sense
Errors should either be undetectable or undoable by the user
Short interactions and understandable and short language in order to avoid being a distraction
Consider Internet/GPS failures and show for example a solution
Respect different screen sizes
Few to no background processes to not drastically affect battery life
Offer data input on a voluntary basis or do not disturb the flow
(cf. Schilling, Apps machen, 45-47)
4. Structure and display information correctly
To ensure that the user is not overwhelmed by information or actions after opening the app, it is important to consider what and when something is displayed. For example, if the goal of the app is to create a new to-do point, this should be immediately executable after opening the app (cf. Schilling, Apps machen, 234). A guideline can be 3 to a maximum of 5 steps to be able to carry out an action. The fewer steps, the better. To take the example of the to-do app again, step one means opening the app, step two would be that the user sees what he wants to do. Step three is that the to-do is saved (cf. Schilling, Apps machen, 239). Another important point is how certain actions that the user can perform are labelled. To give a concrete case study, the magnifying glass as a sign for the search tool. The great advantage for designers is that the use of this symbol without text requires little space. Nevertheless, there are always problems that users have with this sign. Just the sign itself often makes it difficult to find the search function. People start looking in the upper right-hand corner for the search function. If they don’t find it there, they start searching the top of the page. So if the function is poorly labelled, it can quickly lead to frustration. It is also important to mention that using the icon without text adds interaction, as the user has to tap on it, wait for the input field to appear and only then start typing. The realisation is that many symbols still need some kind of label or short description (cf. The Magnifying-Glass Icon in Search Design: Pros and Cons). For another case study, the sidebar in apps. These digital drawers, which can usually be opened by a hamburger menu icon, often tend to be overloaded with rather pointless functions. Problems with this method are also reaching the icon, as it is usually in the upper right or left corner of the screen, there is an additional interaction and the user has to remember which functions are in the sidebar (cf. Li, Please, Don’t Replace the Bar with the Drawer).
5. Smartwatches
Smartwatches play an increasingly important role nowadays and are often an extension of apps. Since the interaction surface is much smaller, it is important to work with high contrast and to display information on a very light or dark background because it is harder to read if the screen size is so small. For Android watches in particular, information should be displayed in the middle, as there is not one watch shape but several. For buttons, the entire width of the interaction area should be used to make interaction easier. Since both Android and Apple have UI guidelines, these should be followed. Especially in terms of font sizes (cf. Schilling, Apps machen, 302).
6. App project phases
These project phases were defined by Karolina Schilling in her book ‘Apps machen’. They have been slightly modified by me to fit our Master’s topic. These project phases are meant to help me to design a good product:
Idea generation & research
Search & find problems
Competition
Solve problems better and create a USP
Target group and market test
Buyer Persona
MVP
Target group
Definition/Research for User Centered Design
Context Scenarios & User Stories
Research
User Personas
User Journeys
Rough conception
Scribbles
Functional requirements
Tap Streams
Concept check
Developer talk
Feature priotisation
Detailed design
Core benefit shibbling
Core benefits wireframes
Prototype core benefits with real visuals or templates
Scribble all other screens, create wireframes, elaborate
Define interactions & transitions and prototype relevant ones
Create and prototype animations
Determine screen transitions
User tests
Tests
User test
Make improvements
Create user interface and deliver graphics
Create and export graphics for the different platforms
Store graphics in a meaningful way
Create visuals for app stores
Design and test user touch points with the app (MVP feedback)
Revang, Magnus. „The User Experience Wheel“ Last modified April 17, 2007. https://userexperienceproject.blogspot.com/2007/04/user-experience-wheel.html
Basecamp. Getting Real, Chicago: Basecamp, (n.d.). Accessed November 09, 2021. https://basecamp.com/gettingreal/09.3-three-state-solution, Three State Solution, chap. 48.
Basecamp. Getting Real, Chicago: Basecamp, (n.d.). Accessed November 09, 2021. https://basecamp.com/gettingreal/09.4-the-blank-slate, The Blank State, chap. 49.
Nielsen Norman Group. „The Magnifying-Glass Icon in Search Design: Pros and Cons“ Last modified February 23, 2014. https://www.nngroup.com/articles/magnifying-glass-icon/
Li, Simon. “Please, Don’t Replace the Bar with the Drawer” Last modified March 31, 2019. http://www.simon-li.com/design-and-code/please-dont-replace-the-bar-with-the-drawer/.
Many people with prosopagnosia (another term is face blindness) use compensatory strategies that help them circumvent their difficulties. There are a few strategies to choose from. But they always have two sides to them. A total of 75 people – people with prosopagnosia, friends or acquaintances and the family of those with the condition – were surveyed through questionnaires and interviews. The following list is intended to show both the positive and negative sides of these methods and what consequences are often involved:
Reliance The method of relying on others is used but is not that popular. It can help if the other person helps to identify people or starts with a conversation during social events. Downside is that it takes a lot of effort, it needs to be discreet and the other person could not always be there to help.
Visual association Only a few people with prosopagnosia stated that they use the strategy to develop memorable links between a persons qualities and character using objects, locations, etc. This requires regular contact and some degree of familiarity with the other person. And some people with DP struggle a lot with visual imagery.
Facial cues to identify This strategy has the most votes and is used the most. Memorising facial features as unusual eyebrows, blemishes or other distinctive features like skin tone can help to identify people. Usually this is done by caricaturing the physical attributes of the face. Downside is that it needs regular contact to maintain the associations and it can be exhausting because it is super effortful, those features must be studied and it can be inappropriate if somebody stars at your mouth during speech for too long.
Identify others through conversation This method is not as often used as distinguishing facial cues. This could be asking to introduce themselves, repeating the name to remember it, introducing first and hoping they would do the same, connecting the topic of the conversation with people they could know, small talk, taking attention to read the other persons reaction and listen to the voice. This strategy could sometimes work but they have to listen more at first to buy the time they need for these cues. This methods has a lot of downsides to it. It can be mentally very exhausting and it is not said that this will reveal who the other person is. Sometimes it can be super inappropriate. People also said that if often seems like they don’t really want to talk and are unwilling to engage in the conversation.
Other cues to identify Other cues than facial ones could be the voice, gait, manners, hairstyle, smell, jewellery, clothes, body shape or posture, character, height, tattoos, ethnicity, gender, glasses, handwriting or bags. Problem is that they can’t trust on this method because everything can suddenly change and some information may not always be shown.
Recognition aids This strategy describes how extra help can lead to identifying persons. This could be through memorising detailed notes on behaviour or appearance, studying photographs, using social media, writing names down during a meeting for example or using name tags. This method can be unreliable as well because people often chance their appearance. The name tag method can work but it is often inappropriate or could be difficult to read.
Avoidance This is a strategy that is not that unusual for people with prosopagnosia. By avoiding uncomfortable situations, using humour to hide difficult or embarrassing moments, avoiding names or being the first person to arrive somewhere some situations can be prevented. But, as all the other strategies as well, this may be inappropriate or undoable. What is worse with this is that it can have serious psychological consequences or can be considered as extremely rude and can lead to hatred or mobbing in the worst case.
Strategies
The following list describes tips and strategies to learn how to deal with prosopagnosia. This list has been compiled by people with this condition and it explicitly states that not all items will fit everyone, but each individual should find his or her own opinion and help. This list is intended to be a guide. (This list was not modified by me in any way)
Social strategies
Avoid referring to people by name or saying anything specific until you are sure you have identified them correctly.
At gatherings where there are some people you know, treat everyone in a friendly way. Smile and say hello to people in passing and this will prevent people thinking you are ignoring them.
When entering into conversation with people you can often work out their identity from what they say.
Look for signs of recognition in people’s body language.
Try to avoid meeting too many people at once.
Ask others to use people’s names when addressing them in your company.
When looking for someone in a group, ask someone you are sure is not the person you’re looking for, such as a person of the opposite sex.
Ask people to introduce themselves every time they see you with their names and how you know each other.
Be careful when visitors come to the door and don’t let people in until you are certain who they are. Other situations may also require caution.
Try to take an interest in people and remember personal details from previous conversations. This can make up for an initial lack of recognition and ensures people don’t think you just aren’t paying attention. This is very difficult if you have memory problems as well, in which case keeping notes on people can help.
Go to parties, meetings or other gatherings with a friend or colleague. Ask the other person to help you identify people before you talk to them.
Get people to wear name tags if appropriate.
Observational strategies
Look at the rings on people’s fingers. A lot of people wear their rings all the time so it can be a reliable way of identifying people in some circumstances, especially if the rings are distinctive.
Look for other jewellery (such as necklaces and bracelets) and distinctive shoes.
Hairstyles are one way of identifying people. This can work well when people have distinctive haircuts, but is less effective for conventional styles. Men are particularly difficult to tell apart by this method.
Walking gaits are very individual, so some people can learn to recognise them effectively.
With practise, people can be easily identifiable by the unique aspects of their accent, speech patterns and turns of phrase.
Look out for distinctive mannerisms, nervous ticks, etc.
Look at body shape and height.
Regular acquaintances can be recognised by their car, bags, or pushchair, etc.
Memory strategies
Invent a mnemonic for remembering someone’s distinctive features, e.g., Dave’s dimples; Pam’s perm. You could even invent ways of remembering people by really mentally exaggerating particular features in the style of a caricature.
Make diagrams and notes of where people are sitting in meetings.
At meetings or parties write down what clothes people are wearing.
Keep a notebook and make notes of people’s identifiable characteristics and features.
Preparation strategies
School teachers can create a seating plan for their classes so they know exactly where everybody is.
You could ask if you can take pictures of people you know so you can study them. Alternatively, facebook and twitter profiles can be very useful. You could add people as friends on facebook and study their profile pictures.
Some photography programmes and computer applications have face recognition technology which can suggest other pictures a person appears in. This can actually help to train you to notice things about a person’s face.
Navigation strategies
Smartphone applications, such as Google Maps, can be invaluable for avoiding getting lost.
Purchase a satellite navigation aid for car journeys.
Learn how to read maps effectively for occasions when Google Maps and satellite navigation aids aren’t available.
Watching movies
Watch TV shows and movies with a friend who can help you identify characters. This also enhances the viewing experience by making it more of a social activity.
Watch films with small casts of characters or one distinctive central character.
The survey also addressed whether disclosure could be of help. In some cases this could be the case, but most would only disclose their condition to people with whom they are in frequent contact. Especially in the workplace, few would disclose their condition because they fear for their personal career security. One point everyone agreed on is that it should be made much more publicly known to the general population as well as to relevant medical professionals in particular, that the condition exists and what consequences it carries with it. Due to the lack of awareness or knowledge of the population, affected people are often portrayed as rude or lazy which can have retroactive negative consequences for the affected people.
All the people involved in this survey were aware of the consequences of this condition. Because there is little information and there are only a few competent and specialized professionals who are trained enough in this field, those affected often get very late, never or a false diagnosis such as autism. Some stated that it would have been much more helpful in dealing with the disorder if they had received a diagnosis earlier. Because of their situation, many were and are not able to understand what is going on with them. By raising awareness and education around said condition, many would have a sense of relief. One other thing that would also help is to create a risk analysis that would record any effective and helpful compensatory strategies. In the end, they often use different methods or strategies depending on the situation they are in and if they have additional help from other people or technology or not.
Sources
Coping Strategies for Developmental Prosopagnosia, Armanda Adams, Peter Hills, Rachel Bennetts, Sarah Bate (06.2019), https://www.researchgate.net/publication/333616235_Coping_strategies_for_developmental_prosopagnosia
Prosopagnosia: face blindness after brain injury, o.A. (2013), https://www.headway.org.uk/media/2816/prosopagnosia-face-blindness-after-brain-injury-factsheet.pdf
One of the most important parts of doing research is hearing the side of the people who have the condition. Below are three stories of people with prosopagnosia.
Story from Walter: “One day […], I saw my brother-in-law from a distance talking with what I thought a little girl. When I got closer, I realized it was my own wife, seriously. Now that is when I realized there was something wrong with me and started checking if there was any online information available. When I found out I suffered from prosopagnosia, it changed my life for the worst because I actually realized that I was greeting people that I thought I recognized and stopped greeting people and avoiding places where I could run into people. I prefer to stay home, instead of going out. […] I don’t have any problem recognizing faces of celebrities and am very good at understanding movie plots. I am really good at remembering locations and always remember how to return from point A to B. I have an excellent short-term memory, yet a bad long-term memory. […].“
Story from Darla: “[…] I took the facial recognition test and realized for the first time that I can’t do something that everyone else can. I was flabbergasted. Over the next several months, memories came flooding back and now they all made sense, all the times I was confused. When I couldn’t find my daughter who was standing literally right beside me. Embarrassing moments in the office when I’m sure I looked like an idiot… all made complete sense. I realized lots of little tricks that I use to recognize when out and about, as I pass people, I look every single person in the eye. I’ve found if you know someone, their face changes – like they brighten up and smile or something. If you don’t know them, they just walk on by. Sometimes it’s tricky, though. They smile just cause they’re friendly and then you get into a conversation with someone, racking your brain trying to figure out who they are, and turns out you don’t. […] And many friends have started saying their name when we get together, which is awesome. But it’s a little annoying when I try to explain it to someone new. 95 percent of the time, they respond by telling me they’re name-blind. Oh, haha, yeah, that’s funny. When I tell them I don’t recognize my own children, they don’t laugh as much. […].”
Story from susieflooze: „I’ve had faceblindness all my life, and it’s a horrible struggle. No one can understand what it’s like when I start to realize the person I’m talking to isn’t whom I think. Suddenly, it feels like the ground under my feet is turning to quicksand as bystanders begin to edge away from me as if I’m insane. It’s impossible to make friends and keep track of them – there’s always the risk of me seemingly snubbing them, and that’s created pain in the past even when the person knew of my condition. They suspect that I must be faking, because how hard is it to simply recognize people?! I can’t help it, and seeing the hurt twinge in their eyes when I introduce myself to people I’ve known for 20 years is like a knife in my guts. I feel sick over it, but I can’t do anything about – all I can do is limit my contacts with people, which is killing me. I live alone and have no one to translate who’s who in my life, and it’s made me a recluse. Even curling up with video is no comfort, because the actors I could recognize have died off or retired, and now I can’t even follow the plot of contemporary movies. I want so badly to connect to the world… but I know all too well it ain’t gonna happen for me. Death will be my only release from this trap. So feel lucky, pilgrim. You have no freakin’ idea how bad this loonytunes brainfart can be.“
Sources
Prosopagnosics Share Their Stories, o.A. (Summer 2019), Face to Face, https://www.faceblind.org/assets/files/newsletters/Face%20to%20Face%20Newsletter%20-%20Summer%202019.pdf
My Life With Face Blindness, susieflooze (2020), https://www.washingtonpost.com/news/magazine/wp/2019/08/21/feature/my-life-with-face-blindness/
Many people who have problems recognizing faces do not know that they suffer from prosopagnosia. There is still a rather limited understanding of this condition among both the general population and the scientific community. However, if a person does not recognize faces well, he or she is usually referred to a neuropsychologist or a researcher. The person is then subjected to some tests and has to answer personal questions on the subject.
Examples of such tests to help diagnose prosopagnosia are:
Recognizing famous faces
Recognizing differences or similarities between two faces
Learning faces and recognizing them later
Recognizing emotion, age and gender
Questions that will be asked are:
Please describe some incidents in which you have been unable to recognize other people.
How do you typically recognize others?
when did you realise that you might have face recognition problems?
Have you ever experienced brain damage, brain surgery, head trauma, amblyopia (lazy eye), strabismus, cataracts early in life, severe untreated myopia, or other serious visual problems?
Do you believe that you have any other face processing difficulties such as reading facial expressions, eye gaze, sex, age, or attractiveness from the face?
do you believe that you have trouble recognising non-facial objects such as cars, animals, or places?
do you believe that your navigational abilities are poor compared to others?
do you think that any of your family members share your difficulties with faces or have other neurological problems?
do you think that you have any other neurological problems?
Sources
face recognition information questions, Brad Duchaine (04.2021), https://www.faceblind.org/research/
Some of the types of therapies are the same or very similar to those used for people with AP (acquired Prosopagnosia). This is a listing of a few of the most common types of therapies:
Comparison of photos of unknown and known faces
Schematic faces, meaning faces reduced to lines
Learning face-name associations
Benton Face Recognition Task in where the participant should identify which face of a selection of faces best matches the target face
Comparison of photos of unknown and known faces with and without hair
Faces that look similar or the same should be matched into pairs
Recognize and distinguish between distorted faces and normal ones
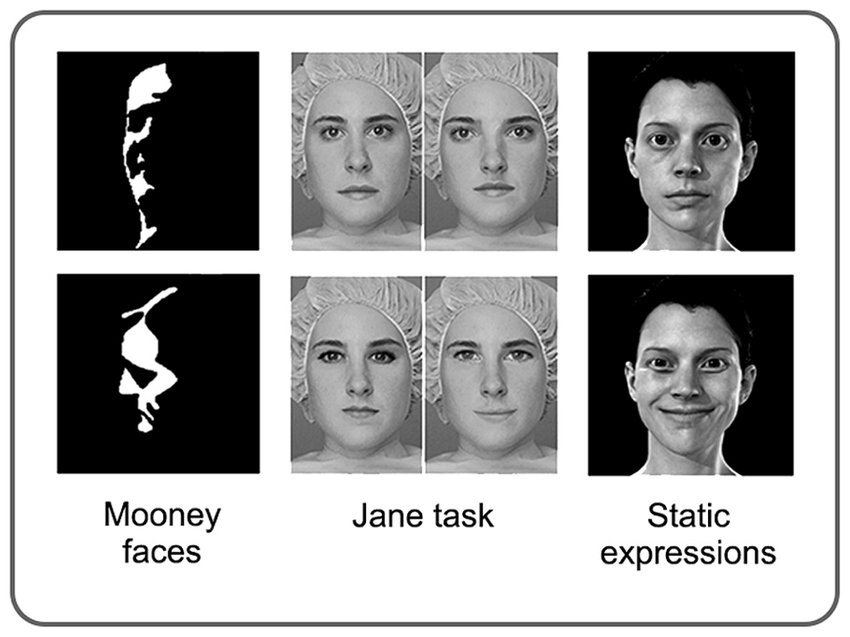
Mooney Faces Task where the face consists only of black and white areas and must be recognized whether it is a face or not
Participants’ attention is drawn to prominent facial features
Two faces are shown and participants should determine age and gender
Faces must be judged by emotions or expressions
Jane Task with detection of spacing, feature, and contour changes
Example of three therapy methods
To give a little more insight into a few of the many types of therapies, here a little more informationen about these methods and what goal should be achieved: One type of compensatory therapy is to learn how to recognize a person’s face based on 5 characteristic features. In this case, the persons are known to the patient. These can be features such as the shape of the face, the width of the nostrils, shape of the eyebrows, freckles or wrinkles. In this way it can be achieved that certain features can be remembered better and therefore it is easier to recognize a person. This kind of therapy brings improvements especially in children. An example of remedial treatment approaches is to divide the face into two areas – distance between eye and eyebrows and mouth and nose – and then categorize them. The goal, after some attempts, should be that people with DP can focus on several features at the same time, allowing them to process rather unfamiliar faces holistically in the brain. Completely different therapeutic approaches have also been tried. For example, it has been found that intranasal inhalation of oxytocin can improve the processing of faces. Oxytocin is a hormone produced in the brain that can influence the processing strategy in the brain. It was also discovered that much more time is spent looking at the eye region. It is believed that the eye region provides important information about who the other person is. This is therefore associated with prosopagnosics, as they spend little time looking at the eye area from the opposite. After giving this hormone and doing various tasks, better performance was observed in some people with DP.
Types of therapies that are most likely to be successful are those where familiar faces are to be learned and recognized using additional information. The goal of these therapies is to eventually be able to better perceive and distinguish facial features, to reduce dependence on certain characteristics or accessories, and to be able to recognize familiar people more likely. However, because these therapies bring little or at least no long-term improvement, it is still advised to use alternative strategies, such as learning how the important people around them talk, walk, or what style of clothing they have. Probably the most important thing is that programs are adapted to the person’s problem, otherwise therapies have little to no success.
Sources
Face Processing Improvements in Prosopagnosia: Successes and Failures over the last 50 years, Joe DeGutis, Christopher Chiu, Mallory E Grosso, Sarah Cohan (8.2014), https://www.researchgate.net/publication/264940858_Face_Processing_Improvements_in_Prosopagnosia_Successes_and_Failures_over_the_last_50_years
Developmental prosopagnosia: A case analysis and treatment study, Lyndsey Nickels, Pamela Joy (09.2006) http://www.researchgate.net/publication/47677051_Developmental_prosopagnosia_A_case_analysis_and_treatment_study
Training of familiar face recognition and visual scan paths for faces in a child with congenital prosopagnosia, Laura Schmalzl, Romina Palermo, Melissa Jayne Green, Ruth Brunsdon (08.2008), https://www.researchgate.net/publication/23187083_Training_of_familiar_face_recognition_and_visual_scan_paths_for_faces_in_a_child_with_congenital_prosopagnosia
There are several types of therapies or programs that are intended to achieve improvements. These types of therapies are used to learn how to work around all the deficits and focus on parts of the face. These are programs that I found during my research, but there are a lot more. So the selection is as follows:
Comparison of photos of unknown and known faces
Learning face-name associations
Identifying which face of a selection of faces best matches the target face
Distinguishing images of real or computer-generated people.
Electrical stimulations
Semantic association chain with additional information about the shown faces
Faces of targets as caricatured versions for recognition
Participants’ attention is drawn to prominent facial features
Only the eye area is shown and participants are asked to say what thoughts and feelings are shown
Two faces are shown and participants should determine age and gender
Faces that look similar or the same should be matched into pairs
According to several studies and a wide variety of tests, the most helpful programs for AP are those that direct attention to prominent facial features, in other words encoding strategies. Age as well as gender, origin or handedness have no effect on whether improvement is possible or not.
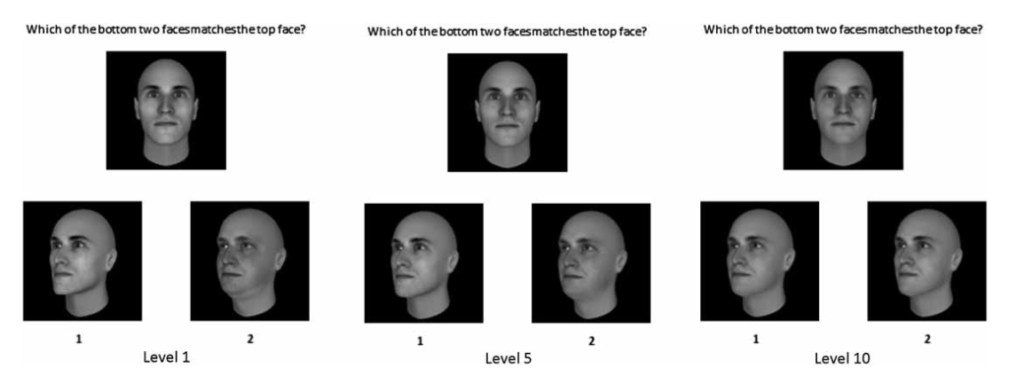
To give a little more insight into one of the many types of therapies, here is one of the methods. A computer game has been developed in which the participant must determine the faces with the greatest similarity to the target face. This game has 10 levels, which become increasingly difficult and challenging depending on the successful completion of the previous levels. Each level consists of searching for a target face from a selection of several faces. The faces searched for were presented frontal or slightly from the side. The further the level, the fewer similarities the faces had with the target face. However, in order to see the first successes, a lot of time must be taken into account. The picture below shows three levels of the game.
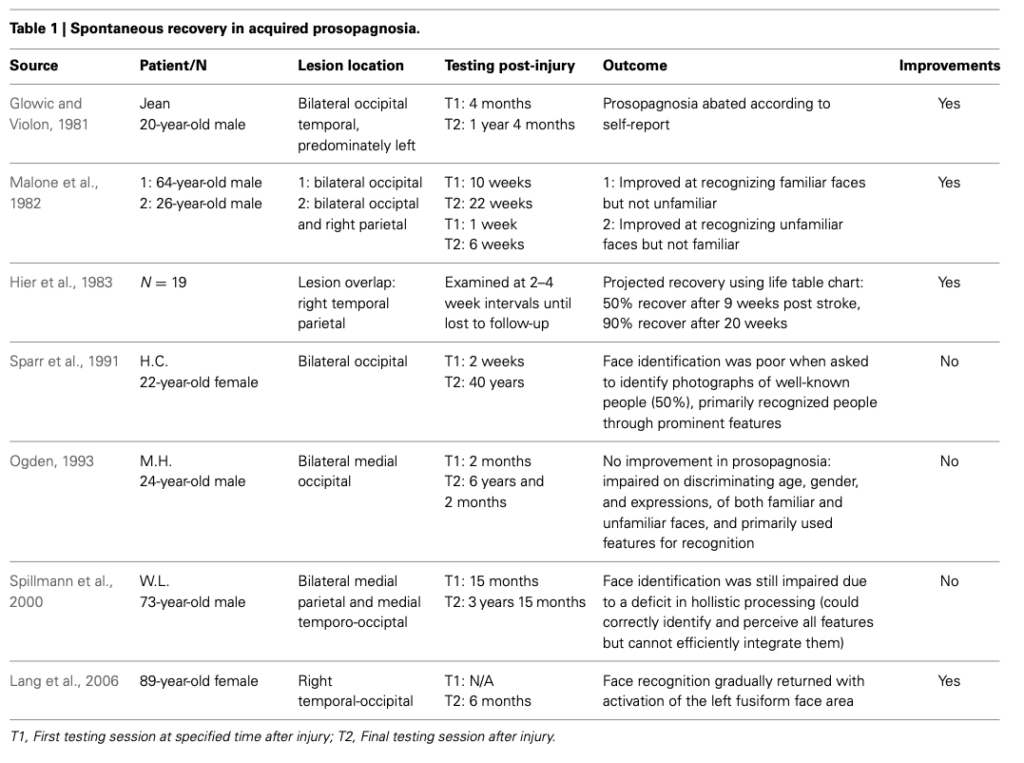
Computer game with 10 different difficulty levels, in which the participant must determine the faces with the greatest similarity to the target face.This table shows a list of participants with AP in therapy programs who either noticed improvements as a result or not.
(Next up in Part 3: Treatment approaches in developmental Prosopagnosia)
Sources
Face Processing Improvements in Prosopagnosia: Successes and Failures over the last 50 years, Joe DeGutis, Christopher Chiu, Mallory E Grosso, Sarah Cohan (8.2014), https://www.researchgate.net/publication/264940858_Face_Processing_Improvements_in_Prosopagnosia_Successes_and_Failures_over_the_last_50_years
Rehabilitation of face-processing skills in an adolescent with prosopagnosia: Evaluation of an online perceptual training programme, Sarah Bate, Rachel Bennetts, Joseph A. Mole, James A. Ainge, Nicola J. Gregory, Anna K. Bobak, Armanda Bussunt (04.11.2019), https://www.researchgate.net/publication/343935303_Prosopagnosia
Short detour into how we humans actually perceive faces
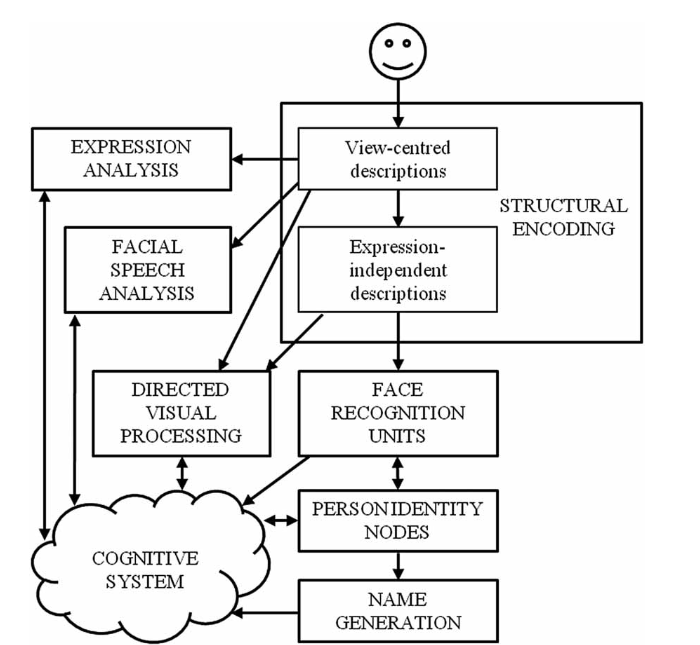
There is a model that describes how we humans perceive faces. It happens in several phases and starts with the brain identifying something that looks like a human face. This is also the phase where we perceive basic visual things like size, figure-ground or orientation. After that, the face is mentally represented while at the same time the brain distinguishes what gender the person is and how old he or she is. In the next phase, the facial features that we perceive are compared with each face that we have stored in our brain and if the face matches we have the feeling that we recognize the person. After these phases we come to the fourth and last phase and we remember the name of the person.
Bruce and Young’s model of face-processing from 1986
Forms and treatments for Prosopagnosia
People with this condition can see every detail of the face. The difference between the brains of these people and people who can recognize faces is that the collected impressions cannot be combined into a complete picture. Since no other cognitive areas in the brain are affected in prosopagnosia, it is not considered a disease. It is more of a dysfunction of the brain, or a genetically determined perceptual weakness. Therefore, the term face blindness is not actually correct, but is still often used to describe this condition.
Once again briefly as a repetition: aquired prosopagnosia develops by for example an accident or as a consequence of an illness, developmental prosopagnosia is since birth and remains in most cases a lifetime. For simplicity, from here on aquired prosopagnosia will be shortened to AP and developmental prosopagnosia to DP.
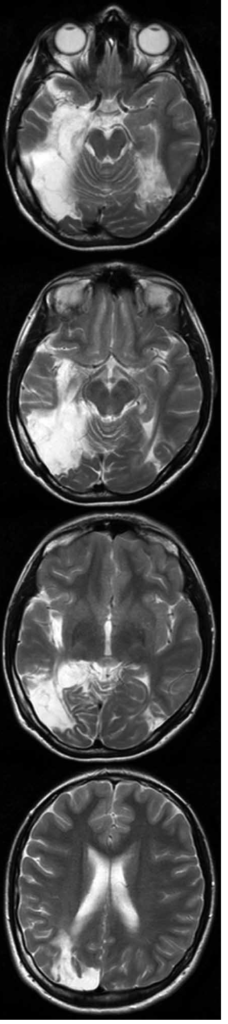
As mentioned in my previous blog post, there is no guarantee of cure. The condition can improve, regardless of age or gender. However, if the damage to the brain is too great, no cure and little to no improvement is possible. Since every condition is different, all training programs must be customized to the person’s needs. Other important points to consider are: does the person only have problems recognizing faces or also objects. In the worst cases – apart from the typical consequences such as anxiety, difficulties with finding and practicing a job or generally social interaction with others – things such as food or doorknobs can no longer be recognized or it is necessary to learn to read and write again.
This image shows a brain scan of a 14 year old girl who was unable to recognize both faces and objects due to a medical condition when she was 8 years old. She had to relearn how to write and read.
There are many training programs that are supposed to help to remember faces or at least to be able to distinguish them. If therapies are actually successful, it is in most cases the fact that these effects do not last long and the therapy must be repeated after a few months. Interestingly, sometimes minor distinctions are made in the programs depending on what form of condition it is. This is because certain mechanisms in the brain, related to face processing, can be modified or changed, at least in people with DP.
Spoiler: Two specific cognitive training programs have been found to work best for AP and DP. One is face morph training and the other is holistic training. These two trainings were the most likely to show improvements.
(Next up in Part 2: Treatment approaches in acquired Prosopagnosia)
Sources
Rehabilitation of face-processing skills in an adolescent with prosopagnosia: Evaluation of an online perceptual training programme, Sarah Bate, Rachel Bennetts, Joseph A. Mole, James A. Ainge, Nicola J. Gregory, Anna K. Bobak, Armanda Bussunt (04.11.2019), https://www.researchgate.net/publication/343935303_Prosopagnosia
Approaches to Improving Face Processing in Prosopagnosia, Joe DeGutis (2016), https://www.cdnetwork.org/wp-content/uploads/2016/12/Degutis_12.13.pdf
Face Processing Improvements in Prosopagnosia: Successes and Failures over the last 50 years, Joe DeGutis, Christopher Chiu, Mallory E Grosso, Sarah Cohan (8.2014), https://www.researchgate.net/publication/264940858_Face_Processing_Improvements_in_Prosopagnosia_Successes_and_Failures_over_the_last_50_years
Face to Face Prosopagnosia Research & Community Spring 2020, o.A. (Spring 2020), https://www.faceblind.org/assets/files/newsletters/Face%20to%20Face%20Newsletter%20-%20Spring%202020.pdf
The term prosopagnosia, also known as face blindness, comes from the Greek and is combined from the words prsosopon for face and gnosis for knowledge. This condition means that people are unable or have difficulty recognizing faces. In other words, identifying or distinguishing people by face is not possible. Prosopagnosia, however, can also affect the ability to recognize objects, places, or cars in some cases. So it is a malfunction of the brain circuits. However, despite having this condition, those with prosopagnosia are neurologically intact and have normal intellectual, socio-cognitive and visual functioning.
These faces are meant to show what some people see who have this condition
Prosopagnosia is estimated to affect approximately 2 percent of the population and is considered a rare disease, as it affects no more or even less than one person in 2,000.
There are two types of prosopagnosia: acquired and developmental or congenital. Acquired means that neurological damage is the trigger, either from a stroke, accident or brain injury. Developmental or congenital means that the affected person has suffered from this disease since early childhood or has inherited it through a genetic connection. Most conditions often originate from birth and it remains for most or the whole lifetime
Managing life with this condition
There is no hope for a cure through specific treatments. That is why those affected often develop their own strategies for dealing with the consequences. To know who the other person is visual or non-visual information is learned. Visual information is body posture or certain characteristics like hairstyle or clothing, non-visual information is the other person’s smell or voice. But these types of strategies will not always work especially in unfamiliar locations or situations.
Cure
As mentioned earlier, there are no treatments that cure the condition. However, there may be techniques that can help some people who have developmental or congenital prosopagnosia to relearn the mechanisms of facial processing again or anew. For people who have this condition due to neurological damage to the brain, certain factors may determine whether recovery can be successful. These include the age of the person when the brain was damaged, the severity of the brain injury, and the timing of treatment.
Problems or consequences of the disease
Prosopagnosia can carry some serious consequences. A person with this disorder may develop an overwhelming fear of social situations and therefore try to avoid social interactions. Consequences may include problems at work and few social contacts. Depression is not an uncommon condition, especially when the condition occurs later in life. Remembering places, distances or orientation points can also be impaired, because this information cannot be processed properly. Some no longer recognize their own face. It is harder to follow plots in movies because the characters are not recognized. Problems such as judging the age or gender of the other person, not being able to follow the gaze or interpret facial expressions are also consequences of this disease. However, this does not always have to be the case. Many can recognize the differences, see if people are laughing for example, but cannot assign this information. A great number of people with this condition report that they fear to appear rude or uninterested, because they do not recognize the other person.
Treatments
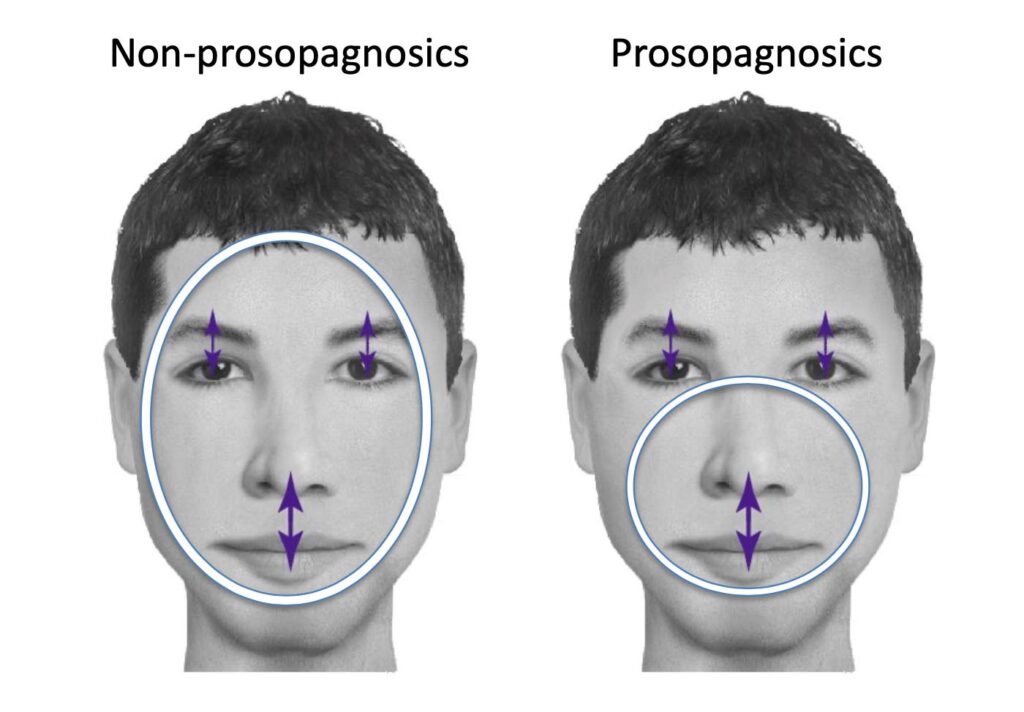
There is a program for people with developmental or congenital prosopagnosia to learn how to recognize faces. The program works by showing computer generated faces of men to the persons with the condition. The task is then to divide these faces into two categories. In one category, the faces must be classified in which the eyebrows and eyes as well as the noses and mouths are closer together. In the other category, the same pairs must be sorted, only the distance is further apart. It is normal to need about two seconds to be able to classify a face. For people with prosopagnosia, it can take six times longer. The purpose behind this cognitive training is to learn not only to remember one particular feature, but to force them to remember the distance between the eyebrows and the eyes, as well as the mouth and nose at the same time. However, this theory does not work for all people with this condition. If these exercises are not continued, it is possible that after about three months this ability to recognize faces will decrease again. Nevertheless, it also shows that it is possible for the brain to acquire new abilities. Researchers believe that it is much easier for younger people to learn or acquire new things, which is why it is advised to start this program relatively early in the hope that the skills will be kept.
Program for people with developmental or congenital prosopagnosia to learn how to recognize faces
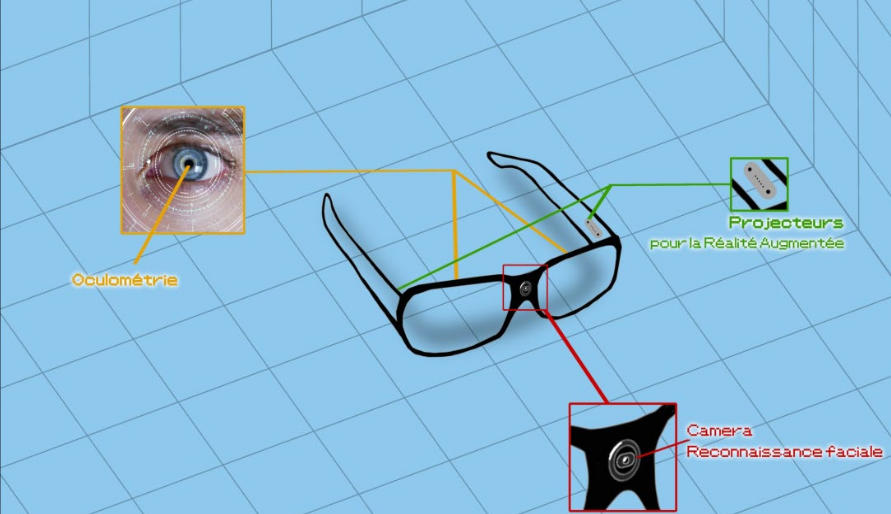
Another tactic comes from seven classmates based in France, who have created a company called CertiFaced to use AR glasses to help people with the condition. The idea is to use software to help identify people by scanning certain distinctive facial features. The principle is intended to work similarly to facial recognition used to unlock cell phones. In order to gain the necessary knowledge, they have talked intensively with this group of people and received a lot of constructive criticism. This project is still in the process of implementation and they hope to get the necessary funding to continue it.
Rare health conditions 31: infantile neuroaxonal dystrophy, progressive hemifacial atrophy, acquired prosopagnosia; and offering emotional and psychological support, Chris Barber (8.1.2020), https://www.magonlinelibrary.com/doi/abs/10.12968/bjha.2020.14.1.15
Prosopagnosia (face blindness), o.A. (last reviewed: 1 May 2019), http://www.nhs.uk/conditions/face-blindness/
Face blindness program shows promise, Mark Roth (1.6.2010), http://www.post-gazette.com/news/health/2010/06/01/Face-blindness-program-shows-promise/stories/201006010140
Can technology help face blindness?, Lam Yee Man Nick (29.10.2019), http://medium.com/@lamyeemanick/can-technology-help-face-blindness-43ce845c9e75
Virtual reality and augmented reality have been increasingly used in healthcare for some time now. Especially in the medical field, this technology is increasingly used to simulate surgeries, to train surgeons or to study the anatomy of the human body in more detail.
War scenario Bravemind
Through VR, veterans can relive fictional war scenarios to confront terrible experiences and overcome post-traumatic stress disorder in a safe environment. As part of their therapy, the veteran is asked to confront their experiences and remember what war was like. The goal of these sessions is to make the remembered scenes more alive and accessible, and to work through them with a therapist. By now it is known that most patients have shown an improvement and reduction of their symptoms.
VR scenario: Bravemind
Training for Surgeries
The surgeon relying entirely on his AR glasses during surgery is still rather unthinkable these days, as technology is involved and failures can occur. However, there are some other ways of using AR glasses that are of great advantage and are already being used in some clinics. By being able to maintain all sterile conditions, they can be used to livestream and record surgeries or communicate with other people outside the operating room. The technology is most likely to be used for teaching and training medical students.
Company: FundamentalVR
VR for people with visual impairments and those who are completely blind
At a conference in 2019, the SeeingVR toolset was introduced. It is intended to enable people who have poor eyesight or are blind to have virtual reality experiences but without having to create extra newly crafted VR experiences. This tool can be overlaid on top of an existing, traditional VR experience as long as the scenario was created using Unity. The tool works in a flexible way to be able to adapt to as many people as possible and to their needs. The user can adjust brightness, zoom in on elements, change contrast or change text color or size. In addition, objects were given brighter edges to highlight them and contours were given to the scene. A laser can be used to point to a text that is then read aloud.
Company: SeeingVR
Embodied Labs to simulate what its like to live with certain health conditions
One company developed labs that use VR simulations to help people experience what it feels like to have certain health conditions. One example of a simulation is Alfred. Alfred is a 74-year-old African-American man who suffers from both high-frequency hearing loss and macular degeneration (a disease of the retina of the eye). Individuals can put on the headset and perceive their surroundings from Alfred’s perspective. Technology is used to increase the volume when a user leans in the direction where the sound is coming from. After a period of time, the user is given a hearing aid to understand what difference the device is making. It is interesting that during tests, even though people read through the introduction, they immediately reported that something has to be broken or that the volume was too low.
Company: Embodied Labs
Children with autism are taught social and communication skills
Floreo is a company that focuses on teaching social and communication skills to autistic children by combining VR with games or other activities and letting them practice certain scenarios. Through this method, children who are often overwhelmed by their real environment can practice and learn to cope in a virtual environment.
Company: Floreo
Detect visual impairments through AR
Using AR glasses and eye tracking, the company SyncThink can determine whether and to what extent visual impairments are present.
Company: SyncThink
Unlearning the sensation of pain
The company Karuna helps people to exercise more to have less pain in their upper body or back. Learned pain or chronic pain is to be unlearned through a 12-week course. Common everyday scenarios or activities must be completed with the help of a VR headset and a tablet with instructions.
Company: KarunaHOME
Improve physical health through VR therapy
Using VR can help people who have psychological problems. An example is fear of heights. Through therapy, a user can be exposed to heights in a protected, simulated environment and learn how to deal with it or try different things. A virtual couch is there to support and help.
Company: Oxford VR
Sources
News Feature: Virtual reality therapy set for a real renaissance, M. Mitchell Waldrop (26.9.2017), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5625944/
Using Google Glass in Surgical Settings: Systematic Review, Nancy J Wie, Bryn Dougherty, Aundria Myers, Sherif M Badawy (6.3.2018), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5861300/
Microsoft Tools Bring VR Access to Low-Vision, Blind Users, Pamela Hogle (10.6.2019), https://learningsolutionsmag.com/articles/microsoft-tools-bring-vr-access-to-low-vision-blind-users?utm_campaign=lspub&utm_medium=link&utm_source=lspub
Can virtual reality change the way we think about health?, Gordon Gottsegen (29.6.2019), https://builtin.com/healthcare-technology/ar-virtual-reality-healthcare
18 Healthcare Augmented Reality and Virtual Reality Companies to Watch, Kayla Matthews (29.6.2020), https://hitconsultant.net/2020/06/29/augmented-reality-and-virtual-reality-companies-to-watch/#.YBBhVS337ow