Some of the types of therapies are the same or very similar to those used for people with AP (acquired Prosopagnosia). This is a listing of a few of the most common types of therapies:
- Comparison of photos of unknown and known faces
- Schematic faces, meaning faces reduced to lines
- Learning face-name associations
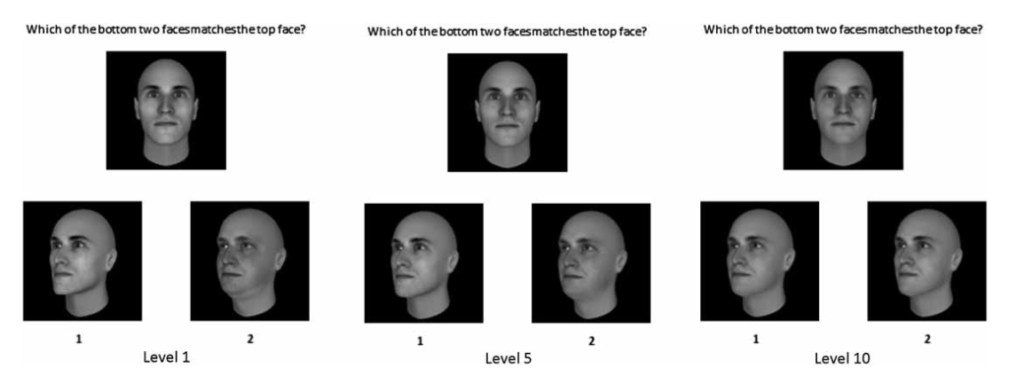
- Benton Face Recognition Task in where the participant should identify which face of a selection of faces best matches the target face
- Comparison of photos of unknown and known faces with and without hair
- Faces that look similar or the same should be matched into pairs
- Recognize and distinguish between distorted faces and normal ones
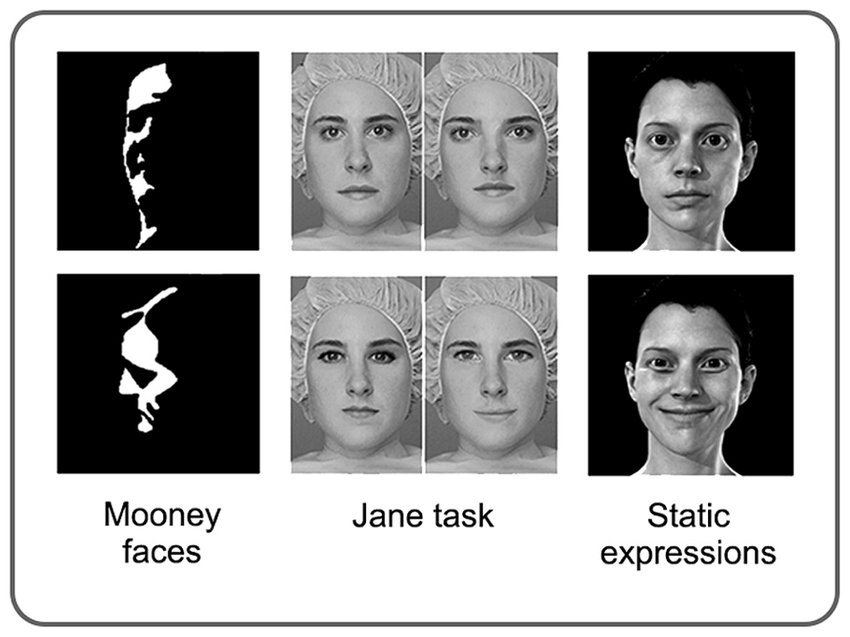
- Mooney Faces Task where the face consists only of black and white areas and must be recognized whether it is a face or not
- Participants’ attention is drawn to prominent facial features
- Two faces are shown and participants should determine age and gender
- Faces must be judged by emotions or expressions
- Jane Task with detection of spacing, feature, and contour changes
To give a little more insight into a few of the many types of therapies, here a little more informationen about these methods and what goal should be achieved:
One type of compensatory therapy is to learn how to recognize a person’s face based on 5 characteristic features. In this case, the persons are known to the patient. These can be features such as the shape of the face, the width of the nostrils, shape of the eyebrows, freckles or wrinkles. In this way it can be achieved that certain features can be remembered better and therefore it is easier to recognize a person. This kind of therapy brings improvements especially in children.
An example of remedial treatment approaches is to divide the face into two areas – distance between eye and eyebrows and mouth and nose – and then categorize them. The goal, after some attempts, should be that people with DP can focus on several features at the same time, allowing them to process rather unfamiliar faces holistically in the brain.
Completely different therapeutic approaches have also been tried. For example, it has been found that intranasal inhalation of oxytocin can improve the processing of faces. Oxytocin is a hormone produced in the brain that can influence the processing strategy in the brain. It was also discovered that much more time is spent looking at the eye region. It is believed that the eye region provides important information about who the other person is. This is therefore associated with prosopagnosics, as they spend little time looking at the eye area from the opposite. After giving this hormone and doing various tasks, better performance was observed in some people with DP.
Types of therapies that are most likely to be successful are those where familiar faces are to be learned and recognized using additional information.
The goal of these therapies is to eventually be able to better perceive and distinguish facial features, to reduce dependence on certain characteristics or accessories, and to be able to recognize familiar people more likely. However, because these therapies bring little or at least no long-term improvement, it is still advised to use alternative strategies, such as learning how the important people around them talk, walk, or what style of clothing they have. Probably the most important thing is that programs are adapted to the person’s problem, otherwise therapies have little to no success.
Sources
- Face Processing Improvements in Prosopagnosia: Successes and Failures over the last 50 years, Joe DeGutis, Christopher Chiu, Mallory E Grosso, Sarah Cohan (8.2014), https://www.researchgate.net/publication/264940858_Face_Processing_Improvements_in_Prosopagnosia_Successes_and_Failures_over_the_last_50_years
- Developmental prosopagnosia: A case analysis and treatment study, Lyndsey Nickels, Pamela Joy (09.2006) http://www.researchgate.net/publication/47677051_Developmental_prosopagnosia_A_case_analysis_and_treatment_study
- Training of familiar face recognition and visual scan paths for faces in a child with congenital prosopagnosia, Laura Schmalzl, Romina Palermo, Melissa Jayne Green, Ruth Brunsdon (08.2008), https://www.researchgate.net/publication/23187083_Training_of_familiar_face_recognition_and_visual_scan_paths_for_faces_in_a_child_with_congenital_prosopagnosia